
2022.12.30
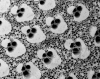
CharXgen活性竹炭包裹在海藻酸鈉微球中作為尿毒症毒素的吸收劑以延緩腎功能惡化新知導讀-CharXgen活性竹炭包裹在海藻酸鈉微球中作為尿毒症毒素的吸收劑以延緩腎功能惡化 by: agnes30 12 月, 2022 本篇文章導讀自: CharXgen-Activated Bamboo Charcoal Encapsulated in Sodium Alginate Microsphere as the Absorbent of Uremic Toxins to Retard Kidney Function Deterioration 以新型活性碳CharXgen餵食CKD大鼠,發現具有保護腎功能及降低血清尿毒症的潛在益處 | 摘要 硫酸吲哚酚 (IS) 和對甲酚硫酸鹽 (PCS) 是慢性腎病 (CKD) 中積累的兩種蛋白質結合尿毒症毒素。本研究的目的是評估新型活性炭 CharXgen 在 CKD 動物模型中對保護腎功能和降低血清尿毒症毒素的影響。 透過掃描電子顯微鏡 (SEM) 和 X 射線衍射儀 (XRD) 對活化前後的CharXgen進行物理特性分析,發現活化後的CharXgen 比表面積增加。 透過體外結合試驗和 CKD 動物模型評估 CharXgen 對生物化學和降低尿毒症毒素的影響。動物試驗總共分成五組,分別是正常組、假手術組(對動物進行和實驗組相同的手術處理,但並不給予實驗刺激)、CKD組、CKD + AST-120組與CKD+CharXgen組。 經掃描電子顯微鏡 (SEM) 和 X 射線衍射儀 (XRD) 分析後發現活化後的CharXgen 具有高內表面積。經體外結核試驗發現CharXgen 能夠有效吸收硫酸吲哚酚及對甲酚硫酸鹽。而在動物實驗中,CKD+CharXgen組的大鼠腎功能獲得改善,且血清中 IS 和 PCS 較低。另外,與 CKD 組相比,發現CKD+CharXgen組的大鼠成纖維細胞生長因子 23 顯著降低,這種變化在CKD + AST-120組未發現。這表明 CharXgen 是一種新型安全無毒的活性炭,具有減輕腎功能惡化和降低與蛋白質結合的尿毒症毒素的潛力。 l 簡介 患有慢性腎病 (CKD) 的患者患心血管疾病 (CVD) 的風險顯著增加,尤其是患有終末期腎病 (ESRD) 的患者。傳統的CVD高風險族群如高血壓、高血脂症和糖尿病患者不能完全解釋CVD增加的風險;而CKD患者這種非傳統的風險因子則有明確的證據支持,其中包括尿毒症毒素的積累、腎功能下降及尿毒症溶質。 尿毒症溶質包括硫酸吲哚酚 (IS) 和對甲酚硫酸鹽 (PCS),它們是腸道菌群代謝芳香氨基酸後源自腸道的兩種蛋白質結合尿毒症毒素,會抑制內皮細胞增殖,可能導致內皮細胞功能的障礙 。而IS 的積累可能會加速腎小球硬化、氧化應激、間質纖維化及腎元減少而促進CKD的進展。IS 參與了 CKD 中 CVD 的發病機制,包括動脈粥樣硬化、外周動脈疾病、充血性心力衰竭、血栓形成和心律失常。另外,成纖維細胞生長因子 23 (FGF23) 是一種從骨分泌的磷酸尿因子,在腎臟功能衰退初期,血中FGF23的濃度即升高。FGF 23 不僅是礦物質骨紊亂的主要調節因子,而且還是導致 CKD 患者心血管發病率和死亡率的因素。因此,減少體內IS 和 PCS的濃度及降低FGF23可能可以延緩CKD的進展。 AST-120 是1991年在日本上市的口服腸道吸附劑,可透過減少 CKD 患者的炎症基因表現,有效降低血清和尿液的 IS 濃度並延緩 CKD 進展的藥物 。在美國的一項初步隨機、雙盲、安慰劑對照試驗中,AST-120 與血清 IS水平的顯著劑量依賴性降低和尿毒症相關不適的減少有關。 因此,通過 AST-120 去除 IS 不僅改善了腎功能,還降低了 CKD 患者心血管事件的風險。 但是AST-120的生產成本較高,所以應用並不廣泛。不過,還有一種從台灣竹子萃取及生產的新型活性炭 CharXgen,具有多孔結構,其安全性、腎臟保護作用以及是否可以降低血清生化指標尚不清楚。因此,作者的目的是研究 CharXgen 對 CKD 動物模型臨床參數的影響。 l 結果 圖 1.掃描電子顯微鏡 (SEM) 分析的竹炭 ( A , B ) 和 CharXgen ( C , D ) 的橫截面和縱截面。 發現Brunauer-Emmett-Teller (BET)比表面積值在竹炭活化過後顯著增加。 圖 2.比較CharXgen及AST-120 在胃腸模擬狀態下吲哚 ( A )、對甲酚 ( B ) 和磷酸鹽 ( C ) 的體外結合能力測定。 在小腸和大腸等條件下,CharXgen 對吲哚的結合親和力更高(圖 2A) 在小腸條件下,CharXgen與對甲酚的結合親和力更高;在大腸條件下,CharXgen 和 AST-120 之間的對甲酚結合親和力沒有顯著差異(圖 2B) 在口腔條件下,CharXgen對磷酸鹽的結合能力與 AST-120 相似;在胃、小腸和大腸條件下,AST-120對磷酸鹽結合能力更高,(圖 2C) 圖 3. 每組大鼠分別在餵食木炭、AST-120 或 CharXgen 後 8、16 和 24 小時的腸道狀態。 結果顯示CharXgen組腸道顏色結果與AST-120組相似,與木炭組相比沒有明顯變黑。 圖 4. 每組大鼠的肝功能和營養狀況。各組GPT( A)和GOT(B)及白蛋白(C)水平無顯著差異。 GPT:谷丙轉氨酶;GOT:谷氨酸草酰乙酸轉氨酶。 CKD + AST-120組 和 CKD + CharXgen 組的肝功能,與正常組或假手術組相比沒有顯著變化(圖 4 A,B) 在血清白蛋白方面,CKD組和CKD+CharXgen組也呈現正常水平(圖4 C) 圖 5. 每組大鼠的腎功能。BUN:血尿素氮;Cr:肌酐 與 CKD 組相比,CKD + CharXgen 組的血清 BUN ( A ) 和 Cr ( B ) 水平顯著降低。 圖 6.每組大鼠的血清鈣 ( A )、磷酸鹽 ( B ) 和 FGF23 ( C ) 水平。(FGF23:成纖維細胞生長因子 23) 每組的鈣和磷酸鹽沒有顯著變化。而在FGF23中顯示CKD + CharXgen 組大鼠的 FGF23 與 CKD 組相比,水平較低。 | 結論 結果顯示 CharXgen新型活性碳具有很大的比表面積及多孔特性,且在體內安全無毒。此外,透過上述實驗發現 CharXgen 在保護大鼠腎功能和降低尿毒症有潛在益處,可能可以減輕 CKD 大鼠腎功能惡化和降低 IS 和、PCS及 FGF23 水平的潛力。不過CharXgen是否在人體腎臟中的具有保護作用還需要再進一步的研究。 l 參考文獻 Vanholder, R.; Massy, Z.; Argiles, A.; Spasovski, G.; Verbeke, F.; Lameire, N.; European Uremic Toxin Work Group. Chronic kidney disease as cause of cardiovascular morbidity and mortality. Nephrol. Dial. Transplant 2005, 20, 1048–1056. [Google Scholar] [CrossRef][Green Version] Levin, A.; Foley, R.N. Cardiovascular disease in chronic renal insufficiency. Am. J. Kidney Dis. 2000, 36, S24–S30. [Google Scholar] [CrossRef] Weiner, D.E.; Tighiouart, H.; Amin, M.G.; Stark, P.C.; MacLeod, B.; Griffith, J.L.; Salem, D.N.; Levey, A.S.; Sarnak, M.J. Chronic kidney disease as a risk factor for cardiovascular disease and all-cause mortality: A pooled analysis of community-based studies. J. Am. Soc. Nephrol. 2004, 15, 1307–1315. [Google Scholar] [CrossRef] Weiner, D.E.; Tighiouart, H.; Elsayed, E.F.; Griffith, J.L.; Salem, D.N.; Levey, A.S.; Sarnak, M.J. The relationship between nontraditional risk factors and outcomes in individuals with stage 3 to 4 CKD. Am. J. Kidney Dis. 2008, 51, 212–223. [Google Scholar] [CrossRef][Green Version] Longenecker, J.C.; Coresh, J.; Powe, N.R.; Levey, A.S.; Fink, N.E.; Martin, A.; Klag, M.J. Traditional cardiovascular disease risk factors in dialysis patients compared with the general population: The CHOICE Study. J. Am. Soc. Nephrol. 2002, 13, 1918–1927. [Google Scholar] [CrossRef][Green Version] Clarke, R.; Daly, L.; Robinson, K.; Naughten, E.; Cahalane, S.; Fowler, B.; Graham, I. Hyperhomocysteinemia: An independent risk factor for vascular disease. N. Engl. J. Med. 1991, 324, 1149–1155. [Google Scholar] [CrossRef] Appel, L.J. Beyond (or Back to) Traditional Risk Factors: Preventing Cardiovascular Disease in Patients with Chronic Kidney Disease. Ann. Intern. Med. 2004, 140, 60–61. [Google Scholar] Sarnak, M.J.; Levey, A.S.; Schoolwerth, A.C.; Coresh, J.; Culleton, B.; Hamm, L.L.; McCullough, P.A.; Kasiske, B.L.; Kelepouris, E.; Klag, M.J.; et al. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Hypertension 2003, 42, 1050–1065. [Google Scholar] [CrossRef] Lin, C.J.; Wu, C.J.; Pan, C.F.; Chen, Y.C.; Sun, F.J.; Chen, H.H. Serum protein-bound uraemic toxins and clinical outcomes in haemodialysis patients. Nephrol. Dial. Transplant. 2010, 25, 3693–3700. [Google Scholar] [CrossRef][Green Version] Dou, L.; Bertrand, E.; Cerini, C.; Faure, V.; Sampol, J.; Vanholder, R.; Berland, Y.; Brunet, P. The uremic solutes p-cresol and indoxyl sulfate inhibit endothelial proliferation and wound repair. Kidney Int. 2004, 65, 442–451. [Google Scholar] [CrossRef] Tumur, Z.; Niwa, T. Indoxyl Sulfate Inhibits Nitric Oxide Production and Cell Viability by Inducing Oxidative Stress in Vascular Endothelial Cells. Am. J. Nephrol. 2009, 29, 551–557. [Google Scholar] [CrossRef] Motojima, M.; Hosokawa, A.; Yamato, H.; Muraki, T.; Yoshioka, T. Uremic toxins of organic anions up-regulate PAI-1 expression by induction of NF-κB and free radical in proximal tubular cells. Kidney Int. 2003, 63, 1671–1680. [Google Scholar] [CrossRef][Green Version] Gelasco, A.K.; Raymond, J.R. Indoxyl sulfate induces complex redox alterations in mesangial cells. Am. J. Physiol. Renal Physiol. 2006, 290, F1551–F1558. [Google Scholar] [CrossRef][Green Version] Ito, S.; Osaka, M.; Higuchi, Y.; Nishijima, F.; Ishii, H.; Yoshida, M. Indoxyl sulfate induces leukocyte-endothelial interactions through up-regulation of E-selectin. J. Biol Chem. 2010, 285, 38869–38875. [Google Scholar] [CrossRef][Green Version] Dou, L.; Burtey, S. The harmful effect of indoxyl sulfate on neovascularization in chronic kidney disease. Kidney Int. 2016, 89, 532–534. [Google Scholar] [CrossRef][Green Version] Lekawanvijit, S.; Kompa, A.R.; Manabe, M.; Wang, B.H.; Langham, R.G.; Nishijima, F.; Kelly, D.J.; Krum, H. Chronic kidney disease-induced cardiac fibrosis is ameliorated by reducing circulating levels of a non-dialysable uremic toxin, indoxyl sulfate. PLoS ONE. 2012, 7, e41281. [Google Scholar] [CrossRef][Green Version] Chitalia, V.C.; Shivanna, S.; Martorell, J.; Balcells, M.; Bosch, I.; Kolandaivelu, K.; Edelman, E.R. Uremic serum and solutes increase post-vascular interventional thrombotic risk through altered stability of smooth muscle cell tissue factor. Circulation 2013, 127, 365–376. [Google Scholar] [CrossRef] Hung, S.C.; Kuo, K.L.; Huang, H.L.; Lin, C.C.; Tsai, T.H.; Wang, C.H.; Chen, J.W.; Lin, S.J.; Huang, P.H.; Tarng, D.C. Indoxyl sulfate suppresses endothelial progenitor cell–mediated neovascularization. Kidney Int. 2016, 89, 574–585. [Google Scholar] [CrossRef][Green Version] Bammens, B.; Evenepoel, P.; Keuleers, H.; Verbeke, K.; Vanrenterghem, Y. Free serum concentrations of the protein-bound retention solute p-cresol predict mortality in hemodialysis patients. Kidney Int. 2006, 69, 1081–1087. [Google Scholar] [CrossRef] Meijers, B.K.; Bammens, B.; De Moor, B.; Verbeke, K.; Vanrenterghem, Y.; Evenepoel, P. Free p-cresol is associated with cardiovascular disease in hemodialysis patients. Kidney Int. 2008, 73, 1174–1180. [Google Scholar] [CrossRef][Green Version] Barreto, F.C.; Barreto, D.V.; Liabeuf, S.; Meert, N.; Glorieux, G.; Temmar, M.; Choukroun, G.; Vanholder, R.; Massy, Z.A.; European Uremic Toxin Work Group (EUTox). Serum indoxyl sulfate is associated with vascular disease and mortality in chronic kidney disease patients. Clin J. Am. Soc. Nephrol. 2009, 4, 1551–1558. [Google Scholar] [CrossRef] [PubMed][Green Version] Lin, C.J.; Wu, V.; Wu, P.C.; Wu, C.J. Meta-Analysis of the Associations of p-Cresyl Sulfate (PCS) and Indoxyl Sulfate (IS) with Cardiovascular Events and All-Cause Mortality in Patients with Chronic Renal Failure. PLoS ONE 2015, 10, e0132589. [Google Scholar] [CrossRef] [PubMed] Gutierrez, O.; Isakova, T.; Rhee, E.; Shah, A.; Holmes, J.; Collerone, G.; Jüppner, H.; Wolf, M. Fibroblast growth factor-23 mitigates hyperphosphatemia but accentuates calcitriol deficiency in chronic kidney disease. J. Am. Soc. Nephrol. 2005, 16, 2205–2215. [Google Scholar] [CrossRef] [PubMed] Lin, C.J.; Pan, C.F.; Chuang, C.K.; Liu, H.L.; Sun, F.J.; Wang, T.J.; Chen, H.H.; Wu, C.J. Association of Indoxyl Sulfate with Fibroblast Growth Factor 23 in Patients with Advanced Chronic Kidney Disease. Am. J. Med. Sci. 2014, 347, 370–376. [Google Scholar] [CrossRef] Isakova, T.; Xie, H.; Yang, W.; Xie, D.; Anderson, A.H.; Scialla, J.; Wahl, P.; Gutiérrez, O.M.; Steigerwalt, S.; He, J.; et al. Fibroblast growth factor 23 and risks of mortality and end-stage renal disease in patients with chronic kidney disease. JAMA 2011, 305, 2432–2439. [Google Scholar] [CrossRef][Green Version] Nakano, C.; Hamano, T.; Fujii, N.; Obi, Y.; Matsui, I.; Tomida, K.; Mikami, S.; Inoue, K.; Shimomura, A.; Nagasawa, Y.; et al. Intactfibroblast growth factor 23 levels predict incident cardiovascular event before but not after the start of dialysis. Bone 2012, 50, 1266–1274. [Google Scholar] [CrossRef] Schulman, G.; Agarwal, R.; Acharya, M.; Berl, T.; Blumenthal, S.; Kopyt, N. A multicenter, randomized, double-blind, placebo-controlled, dose-ranging study of AST-120 (Kremezin) in patients with moderate to severe CKD. Am. J. Kidney Dis. 2006, 47, 565–577. [Google Scholar] [CrossRef] Goto, S.; Kitamura, K.; Kono, K.; Nakai, K.; Fujii, H.; Nishi, S. Association between AST-120 and abdominal aortic calcification in predialysis patients with chronic kidney disease. Clin Exp. Nephrol. 2013, 17, 365–371. [Google Scholar] [CrossRef] Marier, J.F.; Lee, J.; Kambhampati, S.R.; Galitz, L.; Vargas, R.; Moberly, J.; Salazar, D.E. Effect of repeated oral administrations of the oral adsorbent AST-120 on serum creatinine and other markers of renal function. A randomized controlled study in patients with chronic kidney disease. Am. J. Nephrol. 2006, 26, 136–141. [Google Scholar] [CrossRef] Akizawa, T.; Asano, Y.; Morita, S.; Wakita, T.; Onishi, Y.; Fukuhara, S.; Gejyo, F.; Matsuo, S.; Yorioka, N.; Kurokawa, K.; et al. CAP-KD Study Group, Effect of a carbonaceous oral adsorbent on the progression of CKD: A multicenter, randomized, controlled trial. Am. J. Kidney Dis. 2009, 54, 459–467. [Google Scholar] [CrossRef] Fujii, H.; Nishijima, F.; Goto, S.; Sugano, M.; Yamato, H.; Kitazawa, R.; Kitazawa, S.; Fukagawa, M. Oral charcoal adsorbent (AST-120) prevents progression of cardiac damage in chronic kidney disease through suppression of oxidative stress. Nephrol. Dial. Transplant. 2009, 24, 2089–2095. [Google Scholar] [CrossRef][Green Version] Nakai, K.; Fujii, H.; Kono, K.; Goto, S.; Fukagawa, M.; Nishi, S. Effects ofAST-120on left ventricular mass in predialysis patients. Am. J. Nephrol. 2011, 33, 218–223. [Google Scholar] [CrossRef] Vanholder, R.; Smet, R.D. Pathophysiologic effects of uremic retention solutes. J. Am. Soc. Nephrol. 1999, 10, 1815–1823. [Google Scholar] Lin, C.J.; Liou, T.C.; Pan, C.F.; Wu, P.C.; Sun, F.J.; Liu, H.L.; Chen, H.H.; Wu, C.J. The Role of Liver in Determining Serum Colon-Derived Uremic Solutes. PLoS ONE 2015, 10, e0134590. [Google Scholar] [CrossRef] Aronov, P.A.; Luo, F.J.; Plummer, N.S.; Quan, Z.; Holmes, S.; Hostetter, T.H.; Meyer, T.W. Coloniccontribution to uremicsolutes. J. Am. Soc. Nephrol. 2011, 22, 1769–1776. [Google Scholar] [CrossRef][Green Version] Atkinson, S.W.; Young, Y.; Trotter, G.A. Treatment with activated charcoal complicated by gastrointestinal obstruction requiring surgery. BMJ 1992, 305, 563. [Google Scholar] [CrossRef][Green Version] Moe, S.; Drüeke, T.; Cunningham, J.; Goodman, W.; Martin, K.; Olgaard, K.; Ott, S.; Sprague, S.; Lameire, N.; Eknoyan, G.; et al. Definition, evaluation, and classification of renal osteodystrophy: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2006, 69, 1945–1953. [Google Scholar] [CrossRef][Green Version] Parker, B.D.; Schurgers, L.J.; Brandenburg, V.M.; Christenson, R.H.; Vermeer, C.; Ketteler, M.; Shlipak, M.G.; Whooley, M.A.; Ix, J.H. The associations of fibroblast growth factor 23 and uncarboxylated matrix Gla protein with mortality in Coronary artery disease: The heart and soul study. Ann. Intern. Med. 2010, 152, 640–648. [Google Scholar] [CrossRef][Green Version] Gutiérrez, O.M.; Januzzi, J.L.; Isakova, T.; Laliberte, K.; Smith, K.; Collerone, G.; Sarwar, A.; Hoffmann, U.; Coglianese, E.; Christenson, R.; et al. Fibroblast growth factor 23 and left ventricular hypertrophy in chronic kidney disease. Circulation 2009, 119, 2545–2552. [Google Scholar] [CrossRef][Green Version] Fliser, D.; Kollerits, B.; Neyer, U.; Ankerst, D.P.; Lhotta, K.; Lingenhel, A.; Ritz, E.; Kronenberg, F.; MMKD Study Group; Kuen, E.; et al. Fibroblast growth factor 23 (FGF23) predicts progression of chronic kidney disease: The Mild to Moderate Kidney Disease (MMKD) Study. J. Am. Soc. Nephrol. 2007, 18, 2600–2608. [Google Scholar] [CrossRef] Larsson, T.; Nisbeth, U.; Ljunggren, O.; Juppner, H.; Jonsson, K.B. Circulating concentration of FGF-23 increases as renal function declines in patients with chronic kidney disease, but does not change in response to variation in phosphate intake in healthy volunteers. Kidney Int. 2003, 64, 2272–2279. [Google Scholar] [CrossRef][Green Version] Rodelo-Haad, C.; Rodríguez-Ortiz, M.E.; Martin-Malo, A.; Pendon-Ruiz de Mier, M.V.; Agüera, M.L.; Muñoz-Castañeda, J.R.; Soriano, S.; Caravaca, F.; Alvarez-Lara, M.A.; Felsenfeld, A.; et al. Phosphate control in reducing FGF23 levels in hemodialysis patients. PLoS ONE. 2018, 13, e0201537. [Google Scholar] [CrossRef] Francis, C.; David, V. Inflammation regulates fibroblast growth factor 23 production. Curr. Opin. Nephrol. Hypertens. 2016, 25, 325–332. [Google Scholar] [CrossRef][Green Version] Czaya, B.; Faul, C. TheRoleofFibroblast Growth Factor 23 in inflammation and Anemia. Int. J. Mol. Sci. 2019, 20, 4195. [Google Scholar] [CrossRef][Green Version] 文章出處:保健資訊總匯https://drippingpill.com.tw/
2022.06.01
活性碳膠囊與細粒、顆粒差異毒素在小腸末端(ileum)就開始產生及吸收了,還有些吃入的重金屬在胃腸就開始吸收,毒素一般 根本到不了大腸。 細粒附劑顆粒在胃腸是有選擇性的吸附,可以在胃腸就開始吸收毒素,作用比一般膠囊裝活性炭粉在大腸作用更完全。

